Developmental dysplasia of the hip
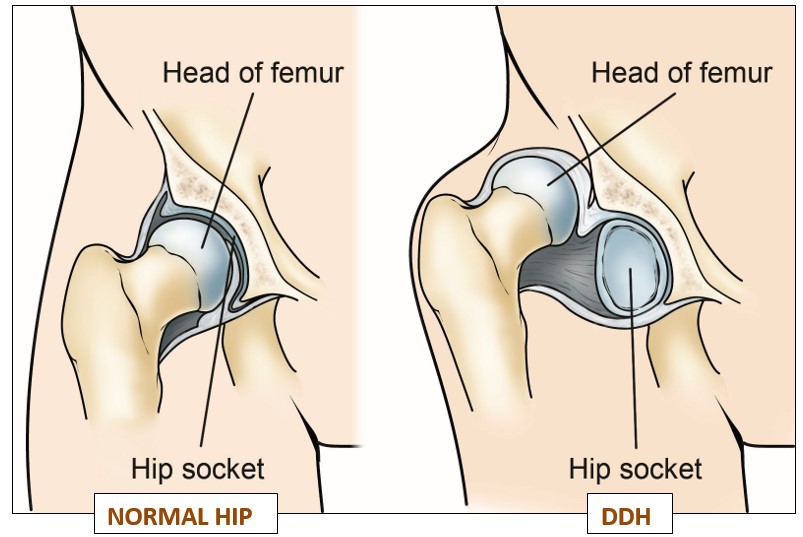
Developmental dysplasia of the hip (DDH) is a condition where the “ball and socket” joint of the hip is not properly formed when the baby is born. It is sometimes called congenital dislocation hip (CDH) or hip dysplasia.
In DDH, the socket of the hip is too shallow and the femoral head is not held tightly in place, so the hip joint is loose. In severe cases, the femur can come out of the socket (dislocation).
DDH may affect one or both hips, but it is more common in the left hip. It is also more common in girls and firstborn children. About 1 or 2 in every 1,000 babies have DDH that needs treatment. Luckily, this condition is less common in India compared to western population.
Without treatment, DDH may lead to problems later in life, including:
* Developing a limp.
* Hip pain –during the teenage.
* Painful and stiff joints (osteoarthritis) in the middle age.
With early diagnosis and treatment, hip joints of most children are able to develop normally.
Diagnosing DDH
* Soon after your baby is born he/she will be examined by the doctor for any birth defects- DDH is one of them. But, as the hip joints are deeply situated, a painless condition like DDH can be very difficult to be diagnosed only with examination by a doctor.
* Ultrasound scan of hip joints is the best test to diagnose DDH in a baby younger than 6 months. An ultrasound scan is usually recommended within a few weeks if:
* The hip feels unstable during initial examination by the doctor
* There is a family history of childhood hip problems
* Problems detected within the uterus of the mother when the baby was within it [like (i) the baby lying bottoms down within the uterus- called breech position (ii) less fluid within the uterus- called oligohydrmnios]
* Baby born with some particular deformities in their feet (Eg. Calcaneovalgus, metatarsus adductus) or neck (Eg. congenital muscular torticollis) indicating that the baby was lying in a cramped uterus.
* After the age of 6 months x rays help to diagnose DDH.
* DDH is not visualised in an antenatal ultrasound scan. (pregnant mother’s scan).
Warning signs of DDH for parents
* Difficulty in separating thighs of the baby for cleaning and putting diapers; one thigh spreads more compared to other.
* One leg (mildly) shorter than the other.
* Delayed onset of walking, which is associated with limping.
Treating DDH
Many times the unstable hip stabilises on its own during first 6 weeks.
Pavlik harness : Babies diagnosed with DDH early in life (less than 6 months of age) are usually treated with a fabric splint called a “Pavlik harness”. This works in two ways: (1) it helps slipped hip to fall back into its socket and (2) it prevents the unstable hip in the socket from slipping again.

The harness position may be confirmed with ultrasound scan or x ray and may be adjusted during follow-up visits.
The harness needs to be worn for several weeks to months. For a baby with complete DDH (hip joint fully out of the socket) this period consists of three phases:
1. Intensive phase: Until the hip joint is reasonably stable (which your doctor can tell you) the harness should not be removed by anyone except a health professional. Usually you need to bring your baby once a week for doctor’s examination and ultrasound scanning/ x ray.
2. Maintenance phase: After the initial ‘stabilizing’ period doctor may permit you to remove the harness during the baby’s bath.
3. Weaning phase: During this, the time for which the harness is worn is gradually reduced.
Other instructions regarding babies on Pavlik harness:
Nappies should be used and they can be worn normally.
Cleaning the harness if it’s soiled – it still should not be removed, but it can be cleaned with detergent and an old toothbrush or nail brush.
Positioning your baby while they sleep – they should be placed on their back and not on their side.
How to help avoid skin irritation around the straps of the harness – you may be advised to wrap some soft, hygienic material around the bands.
Procedures done in the operation theatre
Even after using the Pavlik harness continuously for 3 weeks, if the hip is still lying outside the socket, then harness should be discontinued- otherwise it can lead to complications. In such a situation the ball of hip has to be placed back into its socket (This procedure is called reduction), after giving anaesthesia to the baby in the operation theatre. A large plaster cast called hip spica is put immediately after this to secure the position of the hip joint. Same thing is needed also if your baby is diagnosed with DDH after the age of 6 months.
Reduction may be done as either:
Closed reduction – the ball is placed in the socket without making any large wounds (incisions) over the body. If the hip does not fall back into the socket by closed method, then the surgeon usually decides to do the next higher procedure in the same operation theatre- open reduction.
Open reduction– an incision is made in the groin to allow the surgeon to place the ball in the socket. It is needed in two situations:
Hip does not fall back with closed reduction
Also, if a baby is diagnosed with DDH after 1½ years of age the surgeon may usually decide to do an open reduction.
Care of babies in hip spica:

For most parents, having their baby in a large plaster cast extending from the stomach region to the toes is quite worrisome. The following points may help them:
Toileting care: Hip spica leaves only a small window for the baby’s toileting needs. Parents have to be extra careful while giving toilet care to the baby because if the plaster edges get soaked with urine or motion it cannot be washed off and will stay dirty until the plaster is removed after 6 weeks. This not only leads to ill looking, foul smelling plaster but can cause skin irritation and rashes for the baby also. This window has to be covered with diaper, but if its straps are tied around the hip spica, wet diaper edges soil the plaster. So, parents should use a small/extra small size nappy and its edges should be inserted under the borders of the window in the hip spica.
Body hygiene: With the hip spica on, there is no question of giving bath to the baby!- Parents can only wipe the baby with lukewarm water, making sure no water seeps under the plaster.
Pressure sores: Parents should make sure that, at any point over the edges of the hip spica, it is not in constant contact or pressure over the baby’s skin. Constant pressure or rubbing can lead to sores over the skin.
Make sure no objects go inside the plaster- if trapped in, it can cause sores due to pressure.
Consult your doctor if you have any doubts regarding carrying or handling the baby with hip spica. The baby may have to be taken to the operation theatre after 6 weeks of initial reduction for changing hip spica. This gives opportunity to clean the baby’s skin under cover of the spica, reconfirm the position of the hip joint and to change the plaster to a clean one. The second spica is kept for another 6 weeks. So, altogether the baby will be in hip spica for a period of 12 weeks.
Some additional procedures which are done along with closed/open reduction surgery for DDH:
Adductor tenotomy: In this minor procedure, a tight cord (tendon) on the inner side of the baby’s thigh is partially cut and made lax so that it is easy to reposition the hip to its socket.
K- wire fixation of head of femur: After putting back the ball of hip joint to its socket, the doctor may decide to fix it with a thin metal wire to make sure that it stays in its position. This wire is usually removed after 6 weeks along with spica change.

Before surgery
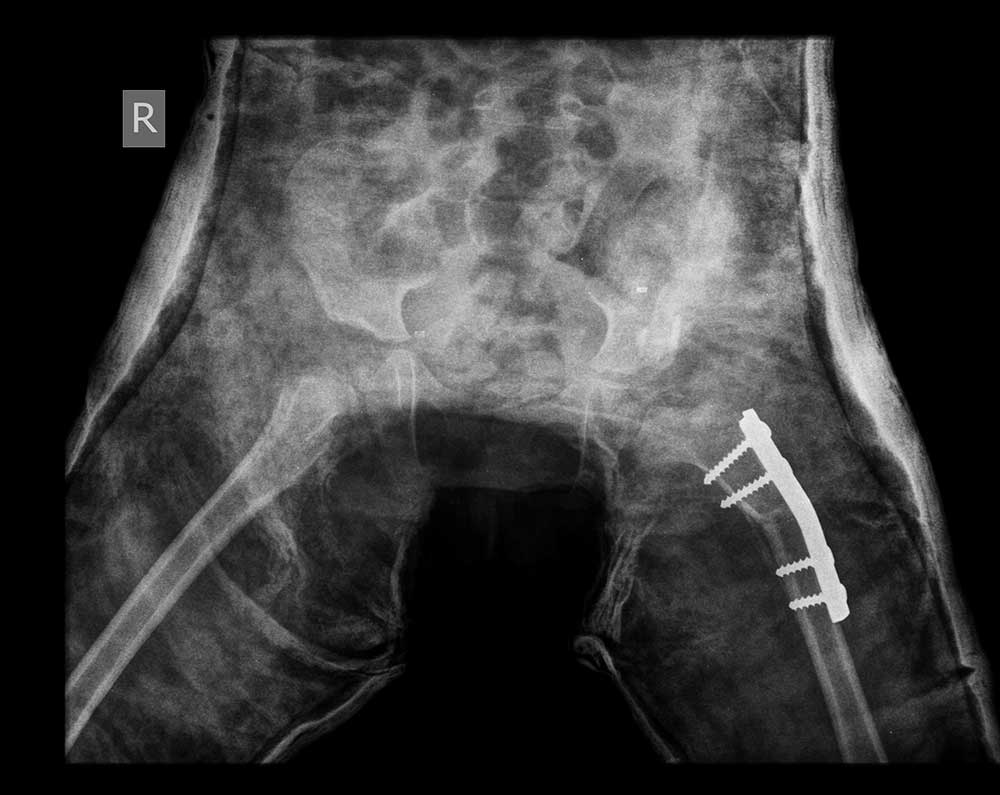
After surgery

Two years After surgery
Osteotomy: If the dislocated hip joint is not corrected at young age, the bones making up the hip joint (upper end of thigh bone and the hip socket) would gradually deform so that even if we just put the ball back into the socket it may not stay there firmly- it will slip out again! To prevent this children older than 1½ years of age, in addition to open reduction the surgeon may cut the deformed bones and re-shape them- this is called osteotomy. DDH is a disease for which early detection and treatment is crucial. As the child becomes older, the grade of treatment becomes higher (more major surgeries are needed) and the results of treatment are less satisfactory even after proper treatment.
Preventing DDH
It’s important to remember DDH cannot be prevented and is nobody’s fault. A baby’s hips are naturally more flexible for a short period after birth. During this time, if your baby spends a lot of time tightly wrapped with their legs straight and pressed together (swaddled), there’s a risk this may slow their hip development. Make sure your baby is able to move their hips and knees freely to kick.